1929 Drinker Respirator
In 1929, Dr. Philip Drinker and pediatric clinician Dr. Charles F. McKhann published an article entitled, The Use of a New Apparatus for the Prolonged Administration of Artificial Respiration: I. A Fatal Case of Poliomyelitis,
that reported successful clinical testing of the Drinker respirator.12
- Image from
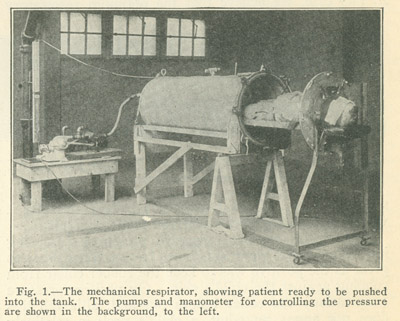
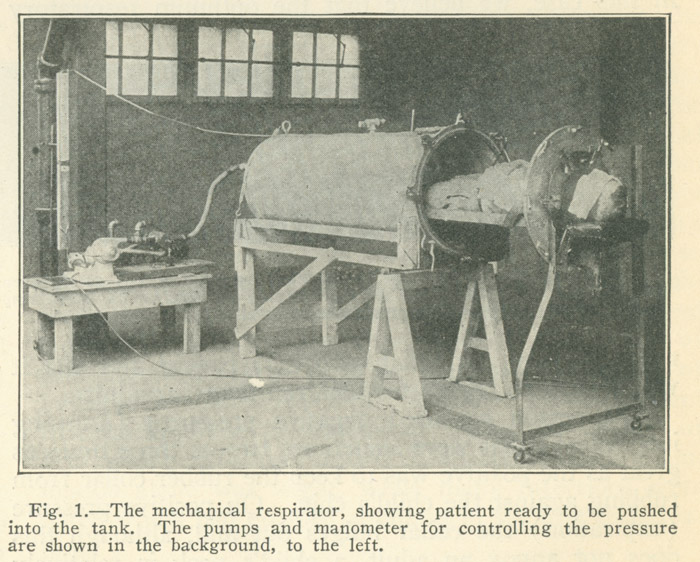
The Use of a New Apparatus for the Prolonged Administration of Artificial Respiration.
The investigators sought to offer all patients suffering from paralytic anterior poliomyelitis the opportunity to recover normal respiration with the assistance of artificial respiration for several hours, several days, or however long might be necessary.
Their study found that manual methods of artificial resuscitation had been ineffective in providing the necessary oxygen interchange and could not be used for extended periods of time. Previous artificial resuscitators, such as the pulmotor, were also poor solutions as their air supplies were too forceful and damaged other organs. Drinker and McKhann outlined several main objectives in their respirator design: long and steady function, adaptability to many ages and sizes, the ability to regulate the rate and depth of respiration, and the ability to provide proper artificial respiration without harming the patient.13
As planned, the Drinker respirator was built to accommodate a full range of patients. It could hold a small child or a fully-grown man as tall as 6 feet 4 inches weighing 225 pounds. The machine satisfied all of the technical goals outlined above, and is still a very functional and accessible respiratory care device.
In using the respirator, the patient lays flat on their back with their head lying on a stand outside of the lid of the tank, with a rubber collar providing a seal around their neck. This rubber collar is designed to offer the seal necessary to maintain a pressurized environment, but still be comfortable for the patient. In this arrangement the medical professionals only have to slide the bed out to examine the patient.
Following the successful testing of the respirator on a human, Consolidated Gas purchased a fully-operable respirator from Harvard and donated it to Bellevue Hospital. Not long after the donation, the respirator provided artificial respiratory support for a patient who was suffering from accidental ingestion of an unknown drug and was unconscious and not breathing. This patient made a full recovery.14
In a historical review, biomedical engineer Philip A. Drinker (son of the iron lung inventor) identifies the Drinker and Shaw iron lung as an early example of biomedical engineering
long before the field was even conceptualized. Drinker suggests that the success of the Drinker and Shaw iron lung can be attributed to the availability of electricity, the immediate need for treatment of polio patients, and the involvement of an engineer in all stages of the device's development.
In this context, it is especially clear why the Drinker iron lung made such a lasting impact upon generations while many comparable devices from decades earlier were almost immediately forgotten.15